

Young Lives research has shown that the COVID-19 pandemic took a toll on young people’s mental health, with a significant decline in subjective well-being and high levels of anxiety and depression (Favara et al., 2022; Porter et al., 2021). By 2023, in India and Peru, anxiety and depression have remained at similar levels, whereas in Ethiopia, anxiety and depression levels have risen, most likely due to the ongoing armed conflict (Quigua et al., 2025). Exposure to multiple crises, exacerbated by the limited capacity of healthcare systems to attend to people with mental health disorders, highlights challenges to achieving Sustainable Development Goal 3.4.: to reduce by one-third premature mortality from non-communicable diseases through prevention and treatment and to promote mental health and well-being by 2030.
Young Lives started measuring young people’s mental health using self-reported scales of anxiety, and depression in 2020-21, in the Round 6 survey, when the two study cohorts were 19-20 years and 26-27 years old. In Round 7, completed during 2023-24, Young Lives collected the same self-reported mental health scales but also hair samples from study participants in Ethiopia, India and Peru to measure cortisol levels, which are correlated with chronic stress.*
This was the first time Young Lives has collected respondents’ hair samples – there are very few longitudinal studies in low- and middle-income countries that have used this method at scale and as part of a longitudinal study. By doing so, Young Lives advanced knowledge of how to implement the collection of large-scale bio-samples in developing countries.
In this blog, we share our planning process, including steps taken to anticipate challenges and maximise participation while considering the future research potential of this data. A full description of the methods implemented and data collection results can be found in Favara et al., 2025, Cortisol Technical Note.
Why collect hair samples to measure mental health?
Cortisol, a hormone found in hair, plays a key role in the body’s response to stressful situations and it has been proven to be an objective and reliable non-invasive measure of chronic stress. Compared to self-reported measures of mental health, measuring hair cortisol is not prone to survey effects, such as desirability bias, where participants answer based on what they think the interviewer wants to hear. Also, a key advantage of measuring hair cortisol rather than other cortisol measurements (for example blood, saliva or urine), is that hair collection does not need to be performed in a laboratory or by a health specialist; it can be done during a regular in-house visit by a trained fieldworker, which facilitates data collection and lowers fieldwork costs.
Strategies to minimise attrition 1: Training the fieldworkers
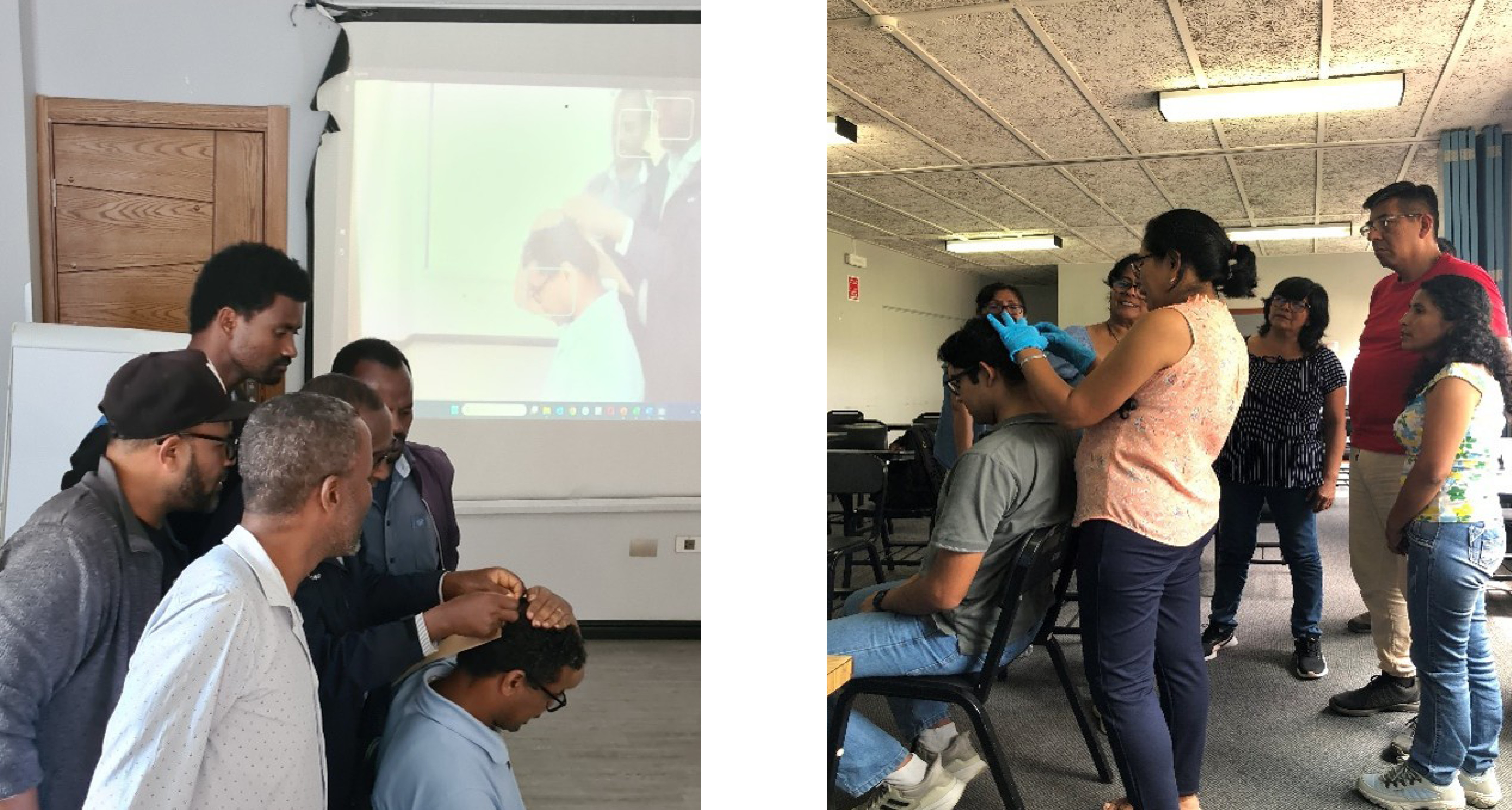
As this was the first time Young Lives had collected hair samples, various training activities were carried out to familiarise fieldworkers with the new procedures and ensure that hair was collected appropriately. The team, together with Sofia Carrera (University of Northwestern) and Katherine Curi (Instituto de Investigación Nutricional), devised training materials on the importance of measuring cortisol for the Young Lives study, how to approach the process of requesting informed consent and how to collect and store hair samples correctly. In each of the three Young Lives countries, specialists provided theoretical and practical training sessions to fieldworkers. The comments and feedback provided (especially by enumerators who have been part of several rounds of the Young Lives study) were crucial to improving the fieldwork manuals. All protocols were also tested as part of the pilots of Round 7 in each country. This was key to anticipating difficulties particular to each country and to preparing fieldworkers to respond to them.
Strategies to minimise attrition 2: Securing informed consent
Collecting hair as part of Round 7 required an additional section in the informed consent form. To gain informed consent, a cornerstone of the Young Lives study, fieldworkers explained to all participants that, in addition to answering the Round 7 survey, they would be asked to provide a lock of hair with the aim of measuring stress among young people. They explained the procedure and showed study participants either a picture of a hair sample (in India and Ethiopia) or an actual hair sample (in Peru) to illustrate the amount of hair to be cut. If participants were uncertain, enumerators showed them a pre-recorded video of the hair sample collection to give a realistic view of what the process would look like. These videos (and hair samples) were particular to each country and gender of the participants.
Challenges encountered and how these were overcome
Despite most participants giving consent to having a hair sample taken, our fieldwork team faced some challenges. Firstly, a minimum hair length of three centimetres is necessary to accurately measure the hair cortisol concentration; the main issue for some was that their hair was too short. This was especially the case for men in Ethiopia. Secondly, in some cases, hair was braided or covered in butter and could not be cut. Where possible, follow-up arrangements were made via phone calls to reconfirm consent and schedule another visit for collection. This approach allowed the hair to reach the necessary length and condition for collection, resulting in a higher success rate in data collection.
Thirdly, as anticipated, some participants expressed doubts about participating in the hair collection component due to cultural or religious reasons, which in some cases led to their refusal to participate in this part of the study. Our protocols were designed to minimise the rate of refusals by enhancing trust and reducing discomfort among participants. The success of these strategies is reflected in the high rates of consent (70% in Ethiopia, 89% in India and 94% in Peru).
Two strategies were crucial to enhance trust. First, the participants’ familiarity with fieldworkers encouraged participation. Second, while the protocols were almost identical for the three countries, additional elements were introduced according to distinctive cultural factors identified. For example, some participants in Ethiopia were concerned about providing a hair sample due to beliefs that hair locks can be used for Satanism or sorcery. Consequently, fieldworkers were prepared to respond to such concerns. Despite adaptations, some cultural and religious reasons prevailed against providing a hair sample, especially in Ethiopia. Finally, some participants refused to take part for aesthetic reasons, thinking that the lack of a hair lock would be visible. To address this concern, the team in Peru used laminated hair samples to show the precise amount of hair required for cortisol analysis. This approach helped obtain consent from participants, as they could see that the amount of hair requested was very small.
Results and looking forward
Overall, our efforts resulted in high rates of hair sample collection. Almost 9 out of 10 participants from India and Peru provided a hair sample. Ethiopia faced a higher proportion of refusals and ineligibilities, resulting in samples being collected from approximately 1 out of 2 participants (Favara et al., 2025, Cortisol Technical Note). As a result, Young Lives collected 5,230 hair samples: 1,935 in Peru, 2,290 in India and 1,005 in Ethiopia, representing the largest hair cortisol collection in low- and middle-income countries as part of a longitudinal study.
Looking forward, hair cortisol will provide an objective measure of the chronic stress faced by young people over the life-cycle. This information will be compared with self-reported mental health to provide a holistic picture of our participants’ well-being. Moreover, it will help us to understand the role of shocks related to Climate Change — as part of the new Young Lives Research Hub on Climate Changes and Environmental Shocks — as well as the impact of armed conflicts, and COVID-19 in shaping different dimensions of mental health over the life-cycle. These rich data will be used to enhance our understanding of the long-term impacts of early-life disadvantages and global crises on stress and how and to what extent mental health relates to health, overall well-being and behaviour in developing countries.
*Unfortunately, Round 7 was not administered in Vietnam due to a change in government procedures for the international transfer of personal data.
References
Favara, M., Hittmeyer, A., Porter, C., Singhal, S., Woldehanna, T., 2022. Young people, mental health, and civil conflict: Preliminary findings from Ethiopia’s Tigray region. Psychiatry Research Communications 2, 100025. https://doi.org/10.1016/j.psycom.2022.100025
Porter, C., Favara, M., Hittmeyer, A., Scott, D., Sánchez Jiménez, A., Ellanki, R., Woldehanna, T., Duc, L.T., Craske, M.G., Stein, A., 2021. Impact of the COVID-19 pandemic on anxiety and depression symptoms of young people in the global south: evidence from a four-country cohort study. BMJ Open 11, e049653. https://doi.org/10.1136/bmjopen-2021-049653
Quigua, J., Favara, M., Sanchez, A., 2025. Young people’s mental health in unprecedented times: research report from round 7 in Ethiopia, India and Peru.
Young Lives research has shown that the COVID-19 pandemic took a toll on young people’s mental health, with a significant decline in subjective well-being and high levels of anxiety and depression (Favara et al., 2022; Porter et al., 2021). By 2023, in India and Peru, anxiety and depression have remained at similar levels, whereas in Ethiopia, anxiety and depression levels have risen, most likely due to the ongoing armed conflict (Quigua et al., 2025). Exposure to multiple crises, exacerbated by the limited capacity of healthcare systems to attend to people with mental health disorders, highlights challenges to achieving Sustainable Development Goal 3.4.: to reduce by one-third premature mortality from non-communicable diseases through prevention and treatment and to promote mental health and well-being by 2030.
Young Lives started measuring young people’s mental health using self-reported scales of anxiety, and depression in 2020-21, in the Round 6 survey, when the two study cohorts were 19-20 years and 26-27 years old. In Round 7, completed during 2023-24, Young Lives collected the same self-reported mental health scales but also hair samples from study participants in Ethiopia, India and Peru to measure cortisol levels, which are correlated with chronic stress.*
This was the first time Young Lives has collected respondents’ hair samples – there are very few longitudinal studies in low- and middle-income countries that have used this method at scale and as part of a longitudinal study. By doing so, Young Lives advanced knowledge of how to implement the collection of large-scale bio-samples in developing countries.
In this blog, we share our planning process, including steps taken to anticipate challenges and maximise participation while considering the future research potential of this data. A full description of the methods implemented and data collection results can be found in Favara et al., 2025, Cortisol Technical Note.
Why collect hair samples to measure mental health?
Cortisol, a hormone found in hair, plays a key role in the body’s response to stressful situations and it has been proven to be an objective and reliable non-invasive measure of chronic stress. Compared to self-reported measures of mental health, measuring hair cortisol is not prone to survey effects, such as desirability bias, where participants answer based on what they think the interviewer wants to hear. Also, a key advantage of measuring hair cortisol rather than other cortisol measurements (for example blood, saliva or urine), is that hair collection does not need to be performed in a laboratory or by a health specialist; it can be done during a regular in-house visit by a trained fieldworker, which facilitates data collection and lowers fieldwork costs.
Strategies to minimise attrition 1: Training the fieldworkers
As this was the first time Young Lives had collected hair samples, various training activities were carried out to familiarise fieldworkers with the new procedures and ensure that hair was collected appropriately. The team, together with Sofia Carrera (University of Northwestern) and Katherine Curi (Instituto de Investigación Nutricional), devised training materials on the importance of measuring cortisol for the Young Lives study, how to approach the process of requesting informed consent and how to collect and store hair samples correctly. In each of the three Young Lives countries, specialists provided theoretical and practical training sessions to fieldworkers. The comments and feedback provided (especially by enumerators who have been part of several rounds of the Young Lives study) were crucial to improving the fieldwork manuals. All protocols were also tested as part of the pilots of Round 7 in each country. This was key to anticipating difficulties particular to each country and to preparing fieldworkers to respond to them.
Strategies to minimise attrition 2: Securing informed consent
Collecting hair as part of Round 7 required an additional section in the informed consent form. To gain informed consent, a cornerstone of the Young Lives study, fieldworkers explained to all participants that, in addition to answering the Round 7 survey, they would be asked to provide a lock of hair with the aim of measuring stress among young people. They explained the procedure and showed study participants either a picture of a hair sample (in India and Ethiopia) or an actual hair sample (in Peru) to illustrate the amount of hair to be cut. If participants were uncertain, enumerators showed them a pre-recorded video of the hair sample collection to give a realistic view of what the process would look like. These videos (and hair samples) were particular to each country and gender of the participants.
Challenges encountered and how these were overcome
Despite most participants giving consent to having a hair sample taken, our fieldwork team faced some challenges. Firstly, a minimum hair length of three centimetres is necessary to accurately measure the hair cortisol concentration; the main issue for some was that their hair was too short. This was especially the case for men in Ethiopia. Secondly, in some cases, hair was braided or covered in butter and could not be cut. Where possible, follow-up arrangements were made via phone calls to reconfirm consent and schedule another visit for collection. This approach allowed the hair to reach the necessary length and condition for collection, resulting in a higher success rate in data collection.
Thirdly, as anticipated, some participants expressed doubts about participating in the hair collection component due to cultural or religious reasons, which in some cases led to their refusal to participate in this part of the study. Our protocols were designed to minimise the rate of refusals by enhancing trust and reducing discomfort among participants. The success of these strategies is reflected in the high rates of consent (70% in Ethiopia, 89% in India and 94% in Peru).
Two strategies were crucial to enhance trust. First, the participants’ familiarity with fieldworkers encouraged participation. Second, while the protocols were almost identical for the three countries, additional elements were introduced according to distinctive cultural factors identified. For example, some participants in Ethiopia were concerned about providing a hair sample due to beliefs that hair locks can be used for Satanism or sorcery. Consequently, fieldworkers were prepared to respond to such concerns. Despite adaptations, some cultural and religious reasons prevailed against providing a hair sample, especially in Ethiopia. Finally, some participants refused to take part for aesthetic reasons, thinking that the lack of a hair lock would be visible. To address this concern, the team in Peru used laminated hair samples to show the precise amount of hair required for cortisol analysis. This approach helped obtain consent from participants, as they could see that the amount of hair requested was very small.
Results and looking forward
Overall, our efforts resulted in high rates of hair sample collection. Almost 9 out of 10 participants from India and Peru provided a hair sample. Ethiopia faced a higher proportion of refusals and ineligibilities, resulting in samples being collected from approximately 1 out of 2 participants (Favara et al., 2025, Cortisol Technical Note). As a result, Young Lives collected 5,230 hair samples: 1,935 in Peru, 2,290 in India and 1,005 in Ethiopia, representing the largest hair cortisol collection in low- and middle-income countries as part of a longitudinal study.
Looking forward, hair cortisol will provide an objective measure of the chronic stress faced by young people over the life-cycle. This information will be compared with self-reported mental health to provide a holistic picture of our participants’ well-being. Moreover, it will help us to understand the role of shocks related to Climate Change — as part of the new Young Lives Research Hub on Climate Changes and Environmental Shocks — as well as the impact of armed conflicts, and COVID-19 in shaping different dimensions of mental health over the life-cycle. These rich data will be used to enhance our understanding of the long-term impacts of early-life disadvantages and global crises on stress and how and to what extent mental health relates to health, overall well-being and behaviour in developing countries.
*Unfortunately, Round 7 was not administered in Vietnam due to a change in government procedures for the international transfer of personal data.
References
Favara, M., Hittmeyer, A., Porter, C., Singhal, S., Woldehanna, T., 2022. Young people, mental health, and civil conflict: Preliminary findings from Ethiopia’s Tigray region. Psychiatry Research Communications 2, 100025. https://doi.org/10.1016/j.psycom.2022.100025
Porter, C., Favara, M., Hittmeyer, A., Scott, D., Sánchez Jiménez, A., Ellanki, R., Woldehanna, T., Duc, L.T., Craske, M.G., Stein, A., 2021. Impact of the COVID-19 pandemic on anxiety and depression symptoms of young people in the global south: evidence from a four-country cohort study. BMJ Open 11, e049653. https://doi.org/10.1136/bmjopen-2021-049653
Quigua, J., Favara, M., Sanchez, A., 2025. Young people’s mental health in unprecedented times: research report from round 7 in Ethiopia, India and Peru.